What is Thyroid Gland
The thyroid gland, for which this classification system is used, is a vital endocrine gland located in the neck that produces hormones regulating metabolism, growth, and development. Its proper function is essential for maintaining overall health, influencing heart, muscle, and digestive function, brain development, and bone maintenance. The thyroid gland produces hormones, primarily thyroxine (T4) and triiodothyronine (T3), which control how quickly the body uses energy, makes proteins, and how sensitive it is to other hormones.
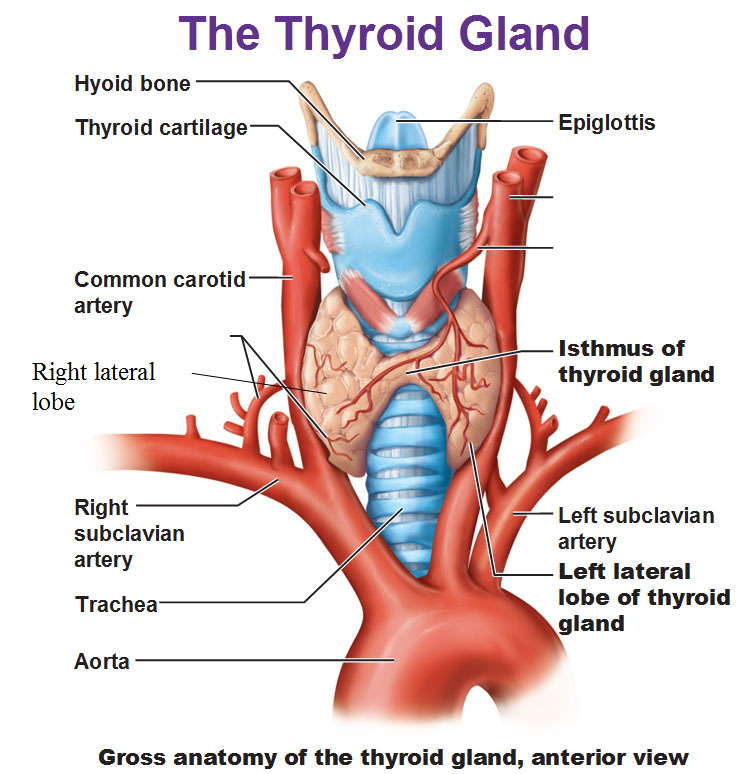

Anatomical Relations:
- Anteriorly:The thyroid gland is covered by the strap muscles (sternohyoid, sternothyroid, and omohyoid) and overlapped by the sternocleidomastoid muscles.
- Posteriorly:It lies adjacent to the larynx and trachea, with the esophagus situated more posteriorly.
- Medially:The thyroid gland is closely related to the larynx and trachea, with the recurrent laryngeal nerves and inferior thyroid arteries located in the tracheo-esophageal groove.
- Laterally:The thyroid gland is adjacent to the carotid sheath containing the common carotid artery and internal jugular vein.
- Superiorly:The superior poles of the thyroid lobes extend up to the level of the thyroid cartilage and are related to the inferior pharyngeal constrictor and cricothyroid muscle.
- Inferiorly:The inferior poles are related to the trachea, recurrent laryngeal nerves, and esophagus.
- Parathyroid Glands:The parathyroid glands are typically located on the posterior surface of the thyroid lobes, within the thyroid capsule.
Important Structures in Relation to the Thyroid:
- Recurrent Laryngeal Nerves:These nerves are closely related to the thyroid gland, particularly in the tracheo-esophageal groove, and are vulnerable to injury during thyroid surgery.
- Inferior Thyroid Artery:This artery typically enters the lower part of the thyroid gland and can have a close relationship with the recurrent laryngeal nerve.
- Superior Thyroid Artery:This artery supplies the superior portion of the thyroid gland and has a close relationship with the superior laryngeal nerve.
- Carotid Sheath:The carotid sheath, containing the common carotid artery and internal jugular vein, lies lateral to the thyroid gland.
Scanning Considerations:
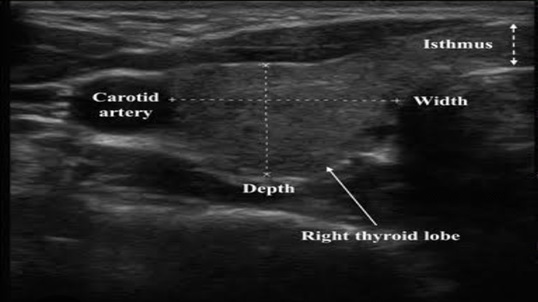
- Ultrasound:Ultrasound is a common imaging modality for visualizing the thyroid gland and surrounding structures.
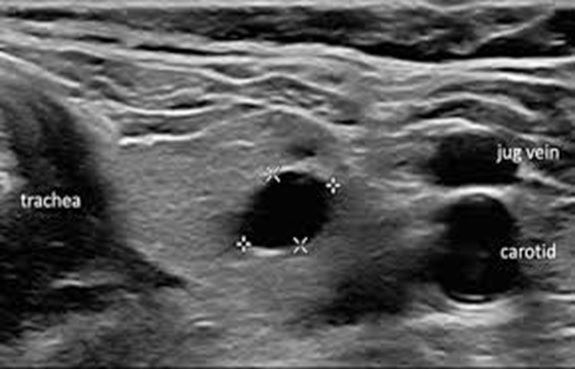
- Landmarks:Key landmarks during ultrasound include the trachea, esophagus, carotid arteries, and jugular veins.
- Transverse and Sagittal Planes:Both transverse and sagittal scanning planes are used to visualize the thyroid lobes and isthmus.
- 3D/4D Ultrasound:3D/4D ultrasound can provide a comprehensive, stereoscopic view of the thyroid gland and its anatomical relationships.
Normal thyroid tissue appears homogeneous and medium-to-high echogenicity. Abnormal findings like nodules, cysts, and other structural changes can be detected based on their appearance and characteristics on the ultrasound.
Appearance: Homogeneous (smooth, uniform), medium- to high-level echogenicity (brightness).
Size and Shape: Varies in the normal population, but generally, the mean length in adults is 40-60mm, and the mean thickness of the lateral lobes is 13-18mm.
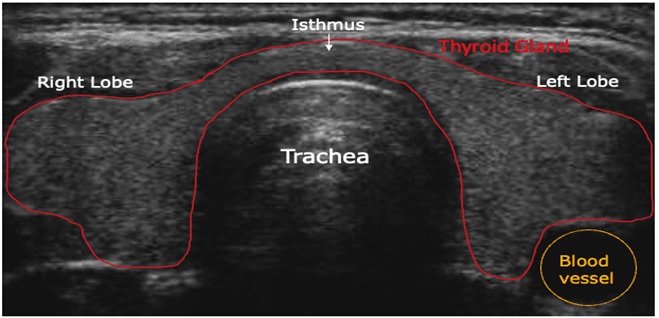
Landmarks of Identifying Structures Surrounding the Thyroid Gland
The trachea, esophagus, blood vessels (carotid arteries and jugular vein), and surrounding muscle groups are key landmarks.

Patient Positioning and Preparation:
1. Positioning: The patient lies on their back with a pillow under their shoulders to extend the neck, exposing the anterior neck.
2. Gel Application: A water-based gel is applied to the anterior neck to ensure good contact between the transducer and the skin.
Scanning Technique:
1. Transducer Selection: A high-frequency linear array transducer (7-12 MHz or higher) is used for detailed imaging.
2. Transverse Scanning:
- Start with the transducer placed transversely (indicator to the patient’s right) over the thyroid gland, starting at the level of the cricoid cartilage.
- Systematically scan the thyroid gland, sliding the transducer laterally to examine each lobe and moving up and down to capture different sections.
3. Longitudinal Scanning:
- Rotate the transducer 90 degrees to a longitudinal orientation (indicator to the patient’s head).
- Scan the thyroid gland from superior to inferior, capturing images of both lobes and the isthmus.
4. Parathyroid Glands:
- When scanning for parathyroid glands, turn the patient’s head slightly to the contralateral side and increase the depth of the image to visualize behind the thyroid gland.
- Dedicated parathyroid images should be obtained, even if no parathyroid tissue is visualized.
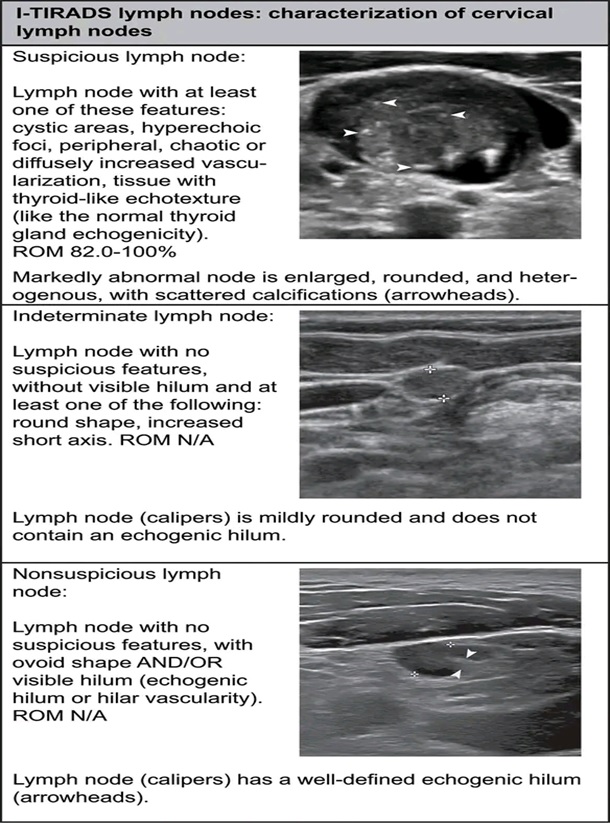
5. Lymph Nodes:
- Scan the lateral neck compartments, including levels 1B, 2, 3, 4, and 5, to assess for abnormal lymph nodes.
- Document any suspicious lymph nodes with measurements and color Doppler imaging.
Documentation and Measurements:
- General Thyroid Images: Obtain transverse and longitudinal images of the right and left lobes, as well as the isthmus.
- Nodules: Measure any nodules in three dimensions and include color Doppler images.
- Lymph Nodes: Measure any suspicious lymph nodes.
- Thyroid Volume: Calculate the volume of the thyroid gland, if needed.
Thyroid ultrasound measurements involve assessing the dimensions and volume of the thyroid gland using ultrasound imaging. Normal thyroid lobe dimensions are typically 4-6 cm in length, 1.3-1.8 cm in anteroposterior (AP) and transverse dimensions, with an isthmus AP dimension of up to 0.3 cm. The normal volume for each lobe is generally considered to be 7-10 mL, with a total thyroid volume (both lobes) of 10-15 mL for females and 12-18 mL for males.
- Document findings: Document all findings, including the size and characteristics of any nodules or lymph nodes, and any other relevant observations.
1B, 2, 3, 4 in thyroid ultrasound reports refers to the risk stratification of thyroid nodules based on ultrasound findings, specifically using the Thyroid Imaging Reporting and Data System (TI-RADS). TI-RADS categorizes nodules from 1 (negative) to 5 (highly suggestive of malignancy), with 1B, 2, 3, and 4 representing varying degrees of suspicion for malignancy.
Breakdown of each category:
TI-RADS 1: Negative for malignancy, with a 0% risk of malignancy.
TI-RADS 2: Benign findings, also with a 0% risk of malignancy.
TI-RADS 3: Probably benign, with a low risk of malignancy (around 1.7%).
TI-RADS 4: This category is further divided:
4a: Low suspicion for malignancy (around 3.3%).
4b: Intermediate suspicion for malignancy (around 9.2%).
4c: Moderate suspicion, but not classic for malignancy (around 44.4-72.4%).
TI-RADS 5: Highly suggestive of malignancy, with a high risk (over 87.5%).
Equipment and Settings:
1. Transducer: Use a high-frequency linear array transducer with appropriate penetration and resolution for the patient’s body habitus.
2. Ultrasound Settings: Optimize the ultrasound settings for thyroid imaging, including focus and depth.
Abnormal Findings
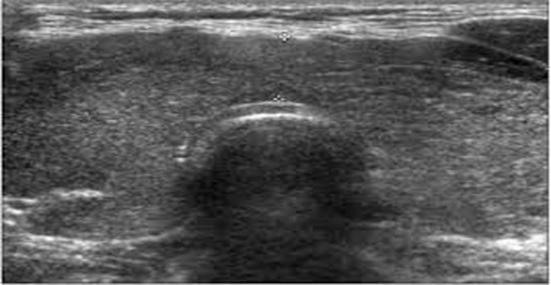
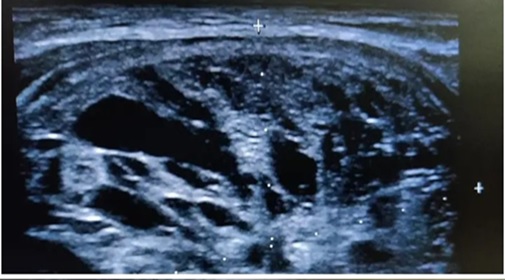
Nodules:
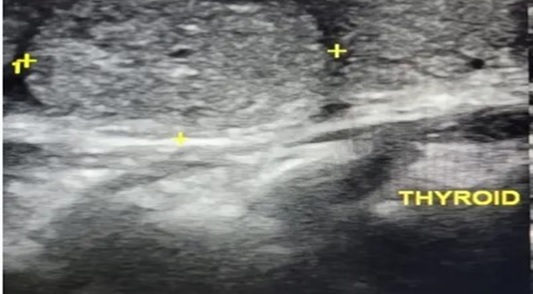
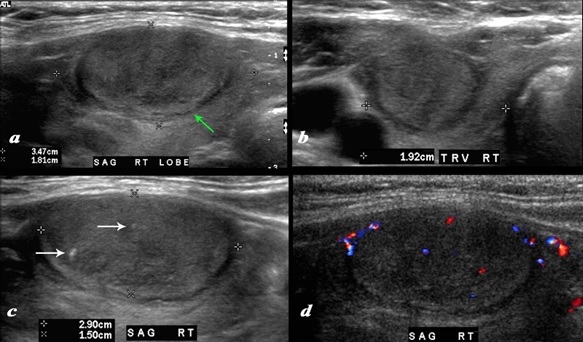
Detection: Ultrasound can identify the presence, site, size, and number of nodules.
Characteristics: Nodules may be solid or contain fluid-filled areas. Some may appear hypoechoic (darker than normal thyroid tissue), while others may be more echo-dense.
SHAPE: May be ovoid or round, with smooth or ill-defined margins.
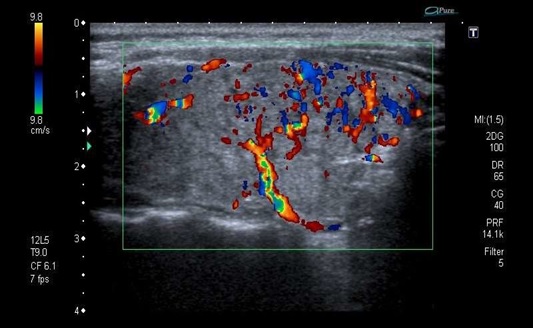
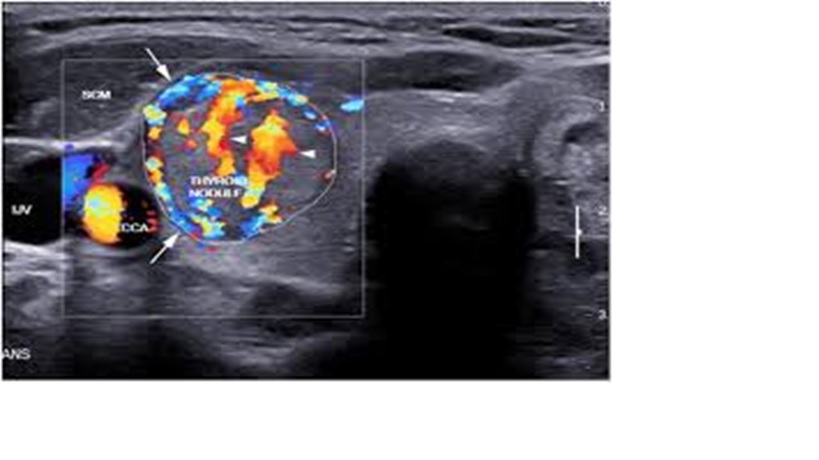
Vascularity
Intranodular vascularization (increased blood flow within the nodule) can be a sign of malignancy.
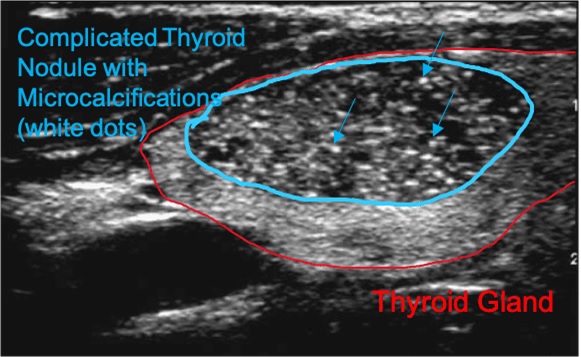
Calcifications
Presence of macro- or microcalcifications can also suggest malignancy.
Cysts
Smooth, globular areas without echoes, often representing epithelial-lined cysts.
Halo
A sonolucent rim (a clear area) around a nodule, potentially indicating a capsule, inflammation, or edema.
Enlargement
A thyroid gland may be considered enlarged if its thickness exceeds 20mm
Other Pathologies Associated With Thyroid Gland
Inflammation, fibrosis, and vascular regions can also manifest as nodule-like structures on ultrasound.
Ultrasonographic Characteristics of Thyroid Nodules
Ultrasound can detect the presence, site, size, and number of thyroid nodules
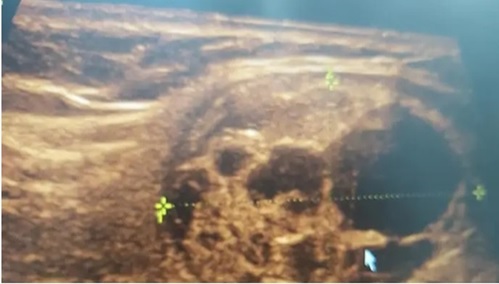
Goiter
A goiter (enlarged thyroid gland) typically appears as a well-defined, often heterogeneous, enlargement of the thyroid gland with multiple nodules. These nodules may contain cystic areas, calcifications, or fibrosis.


Details
Diffuse Enlargement: The thyroid gland lobes are larger than normal, exceeding the upper limits of normal volume (adult males: 12-18 mL, adult females: 10-15 mL). Micronodules (1-7mm).
Nodular Appearance: Multiple nodules of varying sizes are present, indicating a multinodular goiter.
Nodule Characteristics
Solid Nodules: Most nodules are predominantly solid with a smaller cystic component.
Cystic Nodules: Some nodules may have a larger cystic component, often due to colloid, degeneration, hemorrhage, or cystic change.
Halo: A sonolucent (hypoechoic) rim or halo may be seen around nodules, representing a capsule or interface between the nodule and surrounding tissue.
Calcifications: Calcifications are common in goiters and are often coarse and large.
Vascularity: Nodules may show peripheral vascularity on Doppler ultrasound, and hyperfunctioning nodules may have increased intranodular vascularity.
Heterogeneous Appearance: The goiter’s appearance on ultrasound is often heterogeneous due to the presence of different nodule types, calcifications, fibrosis, cystic changes, and hemorrhage.
How to Measure The Thyroid Lobes
Spongiform/Honeycomb Pattern
Some nodules may show a spongiform or honeycomb pattern, often associated with colloid.
Colloid
Colloid nodules may have tiny echogenic foci with comet-tail artifacts.
Clinical Significance
Diagnosis: Ultrasound is a valuable tool for diagnosing and characterizing goiter, including the presence and characteristics of nodules.
A risk assessment: Ultrasound helps assess the risk of malignancy in thyroid nodules, especially when combined with other clinical factors.
Guidance for Biopsy: Ultrasound can guide fine-needle aspiration (FNA) biopsies of thyroid nodules, which is essential for definitive diagnosis.
Monitoring: Ultrasound can be used to monitor goiter size and nodule characteristics over time.
Characterization of Goiter
Several ultrasound features are used in charactrizing, they include:
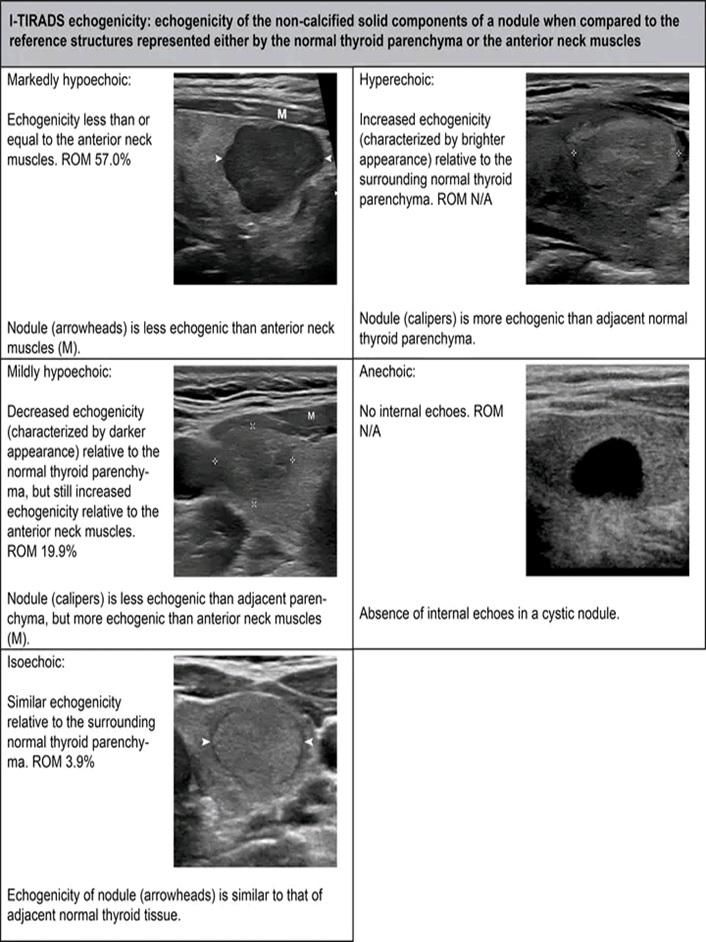
Echogenicity: Whether the nodule is hypoechoic (darker than surrounding tissue), isoechoic (similar to surrounding tissue), or hyperechoic (brighter).
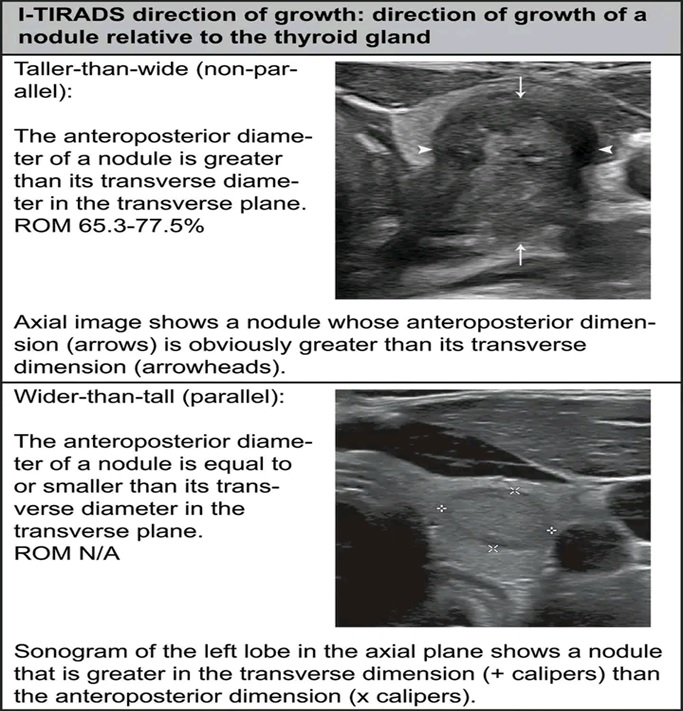
Shape: Ovoid, round, or taller-than-wide shapes are considered.
Margins: Smooth, irregular, or spiculated margins can indicate malignancy.
Calcifications: Microcalcifications (small, bright spots), macrocalcifications, and rim calcifications are assessed.
Size: The size of the nodule is an important factor in determining the need for further investigation, such as biopsy.
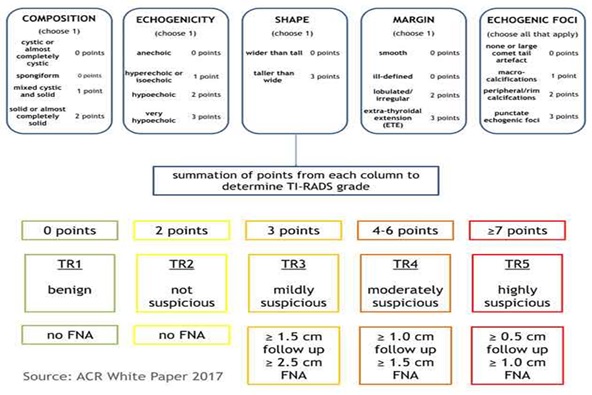
Scoring is determined from five categories of ultrasound findings.the higher the cumulative score, the higher the tr (ti-rads) level and the likelihood of malignancy.
One score is assigned from each of the following categories:
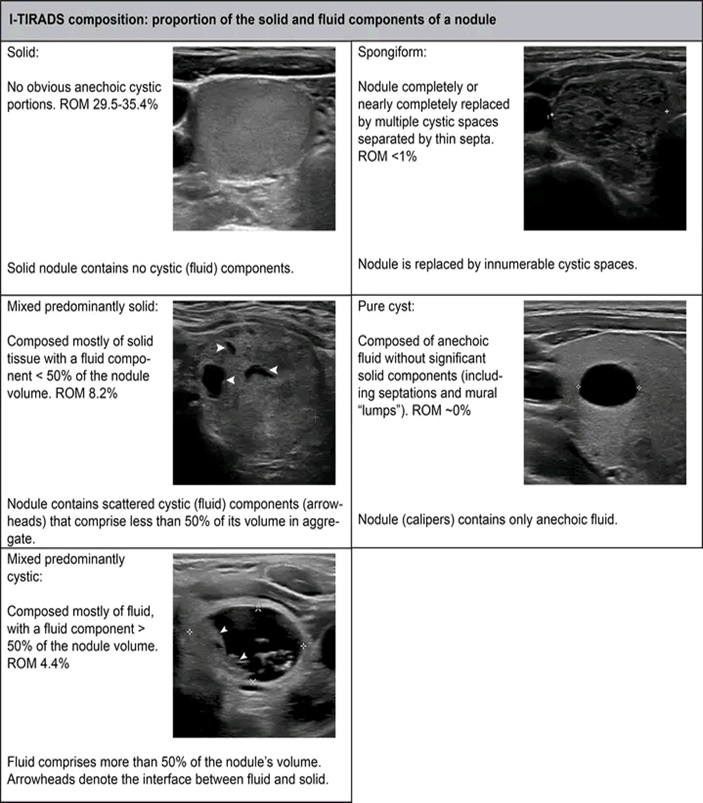
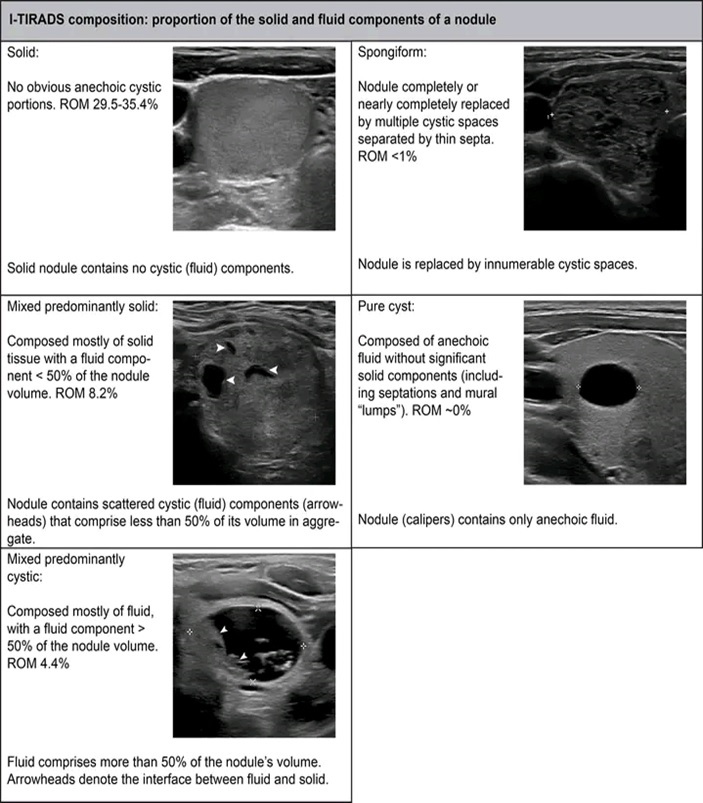
Composition: (choose one)
- cystic or completely cystic *: 0 points
- spongiform *: 0 points
- mixed cystic and solid: 1 point
- solid or almost completely solid: 2 points
Echogenicity: (choose one)
- anechoic: 0 points
- hyper- or isoechoic: 1 point
- hypoechoic: 2 points
- very hypoechoic: 3 points
Shape: (choose one) (assessed on the transverse plane)
- wider than tall: 0 points
- taller than wide: 3 points
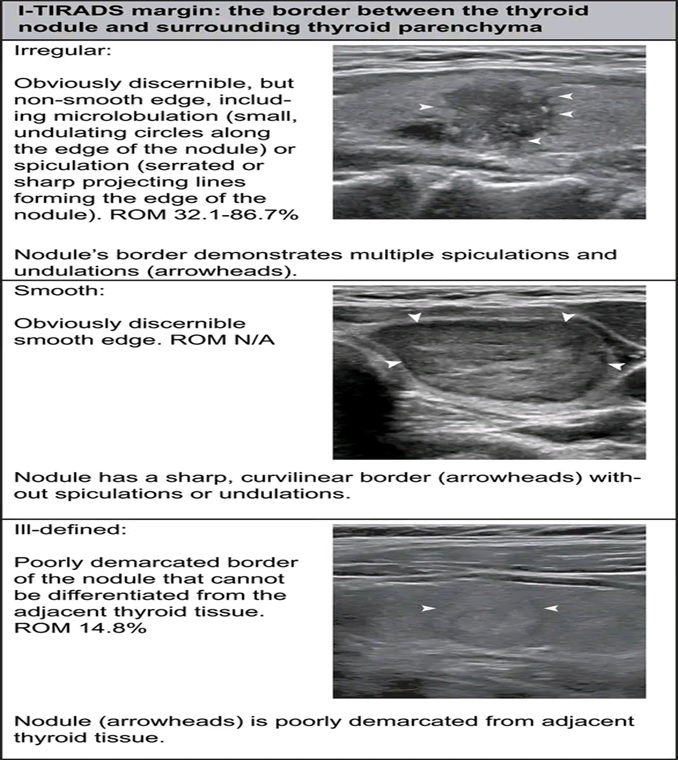
Margin: (choose one)
- smooth: 0 points
- ill-defined: 0 points
- lobulated/irregular: 2 points
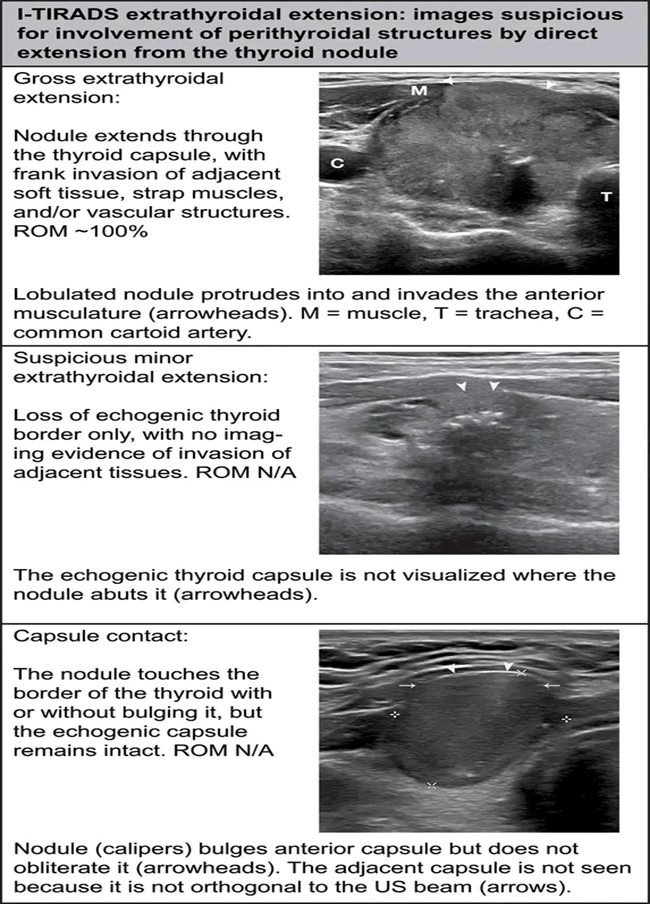
- extra-thyroidal extension: 3 points
Any and all findings in the final category are also added to the other four scores.
Echogenic foci: (choose one or more)
- none: 0 points
- large comet-tail artifact: 0 points
- macrocalcifications: 1 point
- peripheral/rim calcifications: 2 points
- punctate echogenic foci: 3 points
List of Thyroid Pathologies
- 1. GOITER
- 2. GRAVES DISEASE
- 3. HASHIMOTO THYROIDITIS
- 4. BENIGN THYROID NODULES