Scanning protocol for the liver
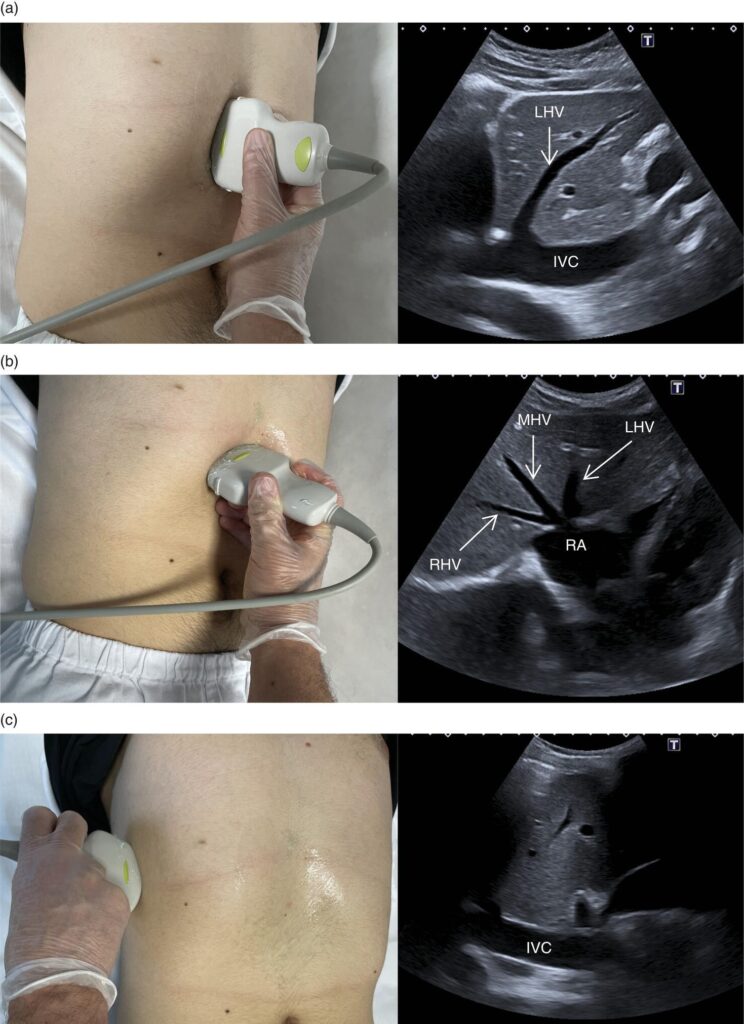
The subcostal approach for liver ultrasound involves positioning the ultrasound probe beneath the rib cage to visualize the liver.This technique is particularly useful for imaging the right lobe and the superior aspects of the liver, especially when the patient is holding their breath.
Detailed Steps:
- Patient Positioning: The patient typically lies supine (on their back).
- Probe Selection: A curvilinear or phased-array transducer is commonly used.
- Probe Placement: The probe is placed subcostally, typically in the midline or slightly to the right of the midline, just below the xiphoid process.
- Initial View: The initial view is often a transverse (cross-sectional) view of the liver.
- Deep Inspiration: The patient is instructed to take a deep breath and hold it. This helps to depress the liver, bringing it closer to the probe and improving visualization.
- Scanning Technique: The transducer is then swept in a fan-like motion, angling the probe slightly up and down to visualize different sections of the liver, including the right and left lobes.
- Intercostal Scanning: The probe is then moved to the intercostal spaces (between the ribs) to further assess the liver, particularly the posterior aspects of the right lobe.
- Right Lateral Decubitus Position: In some cases, the patient may be rolled onto their left side (right lateral decubitus position) to improve visualization of the right lobe and gallbladder.
- Additional Views: Sagittal (longitudinal) views are also obtained to visualize the liver in a different plane.
- Color Doppler: Color Doppler may be used to assess blood flow in the hepatic vessels.
Tips for Optimal Visualization:
- Deep Inspiration:Deep breaths help to bring the liver into better view by displacing air-filled bowel.
- Patient Positioning:Slight adjustments to patient positioning, such as rolling them onto their side, can improve visualization.
- Intercostal Scanning:Utilizing intercostal spaces can help overcome limitations of the subcostal approach.
- Bowel Gas:Bowel gas can obscure the view of the liver. Distending the abdomen or using other maneuvers may help minimize its effects.
- Fasting:Avoiding eating or drinking for several hours before the scan can help reduce gas and improve visualization.
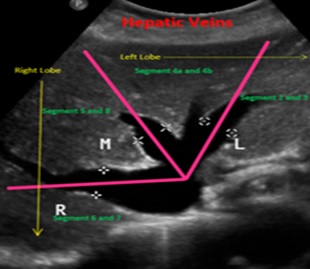
Brief Sonographic Anatomy of the Liver
The right,middle,and left hepatic veins divide the liver into sectors and segments,with the right hepatic vein dividing the lobe into anterior and posterior segments,and the left hepatic vein dividing the left lobe into medial and lateral segments. These veins drain into the inferior vena cava (IVC).
Key Points:
- Hepatic Vein Location:The hepatic veins (right, middle, and left) are located in the posterosuperior aspect of the liver and drain into the IVC.
- Segmental Anatomy:The right hepatic vein marks the boundary between the right anterior and posterior segments. The middle hepatic vein divides the liver into right and left lobes. The left hepatic vein, along with the umbilical fissure and falciform ligament, divides the left lobe into medial and lateral segments.
- Caudate Lobe:The caudate lobe, a separate segment, is located posteriorly and drained by several small hepatic veins that enter the IVC directly.
- Sonographic Appearance:Hepatic veins appear as anechoic (dark) tubular structures within the liver parenchyma, in contrast to the portal veins which have bright echogenic walls.
Glisson’s capsule: A fibrous layer covering the liver, which extends into the liver structure and supports the blood vessels, ducts, and nerves.
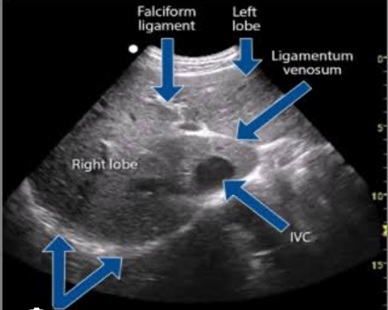
Hepatic ligaments
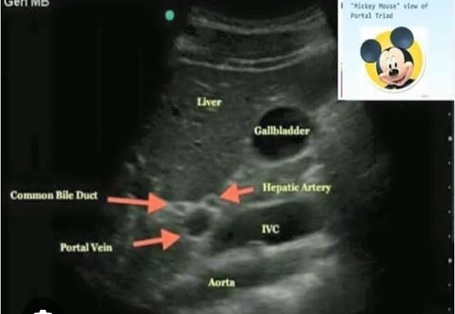
Porta hepatis: The area on the visceral surface of the liver where blood vessels, bile ducts, and nerves enter.
Falciform ligament: A ligament that separates the right and left lobes of the liver.
Coronary ligament: A ligament that attaches the liver to the inferior surface of the diaphragm.
Ligamentum venosum: A remnant of the embryonic ductus venosus, which separates the caudate lobe from the left lobe.
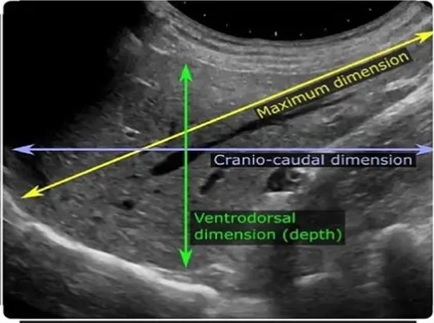
How to Measure the Liver Dimensions
Hepatic Segments
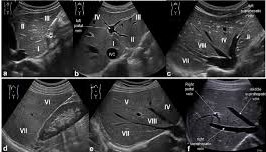
The liver is sonographically divided into segments based on the Couinaud’s classification, which utilizes the branches of the portal vein, hepatic veins, ligaments, and fissures as landmarks. This segmentation is clinically relevant for planning liver resections and localizing tumors.
- Medial and Lateral Segments:
The left lobe is divided into medial (segment IV) and lateral (segments II and III) segments by the falciform ligament.
II. The Eight Segments (S1-S8):
The caudate lobe
- Segment I (Caudate Lobe): Located posteriorly between the fissure for the ligamentum venosum and the inferior vena cava.
- Segments II and III (Left Lateral): Located laterally to the falciform ligament, with segment II superior and segment III inferior to the portal venous supply.
- Segment IV (Left Medial): Located medial to the falciform ligament.
- Segments V and VI (Right Anterior): Located anterior to the right hepatic vein.
- Segments VII and VIII (Right Posterior): Located posterior to the right hepatic vein.
III. Key Landmarks for Sonographic Identification:
- Branches of the Portal Vein: These are crucial for defining the boundaries between segments.
- Hepatic Veins: The right, middle, and left hepatic veins help delineate the lobes and segments.
- Ligaments and Fissures: The falciform ligament and other fissures help define the boundaries of the left lobe segments.
- Gallbladder: The gallbladder fossa helps define the right lobe.
Simple Hepatic Cyst
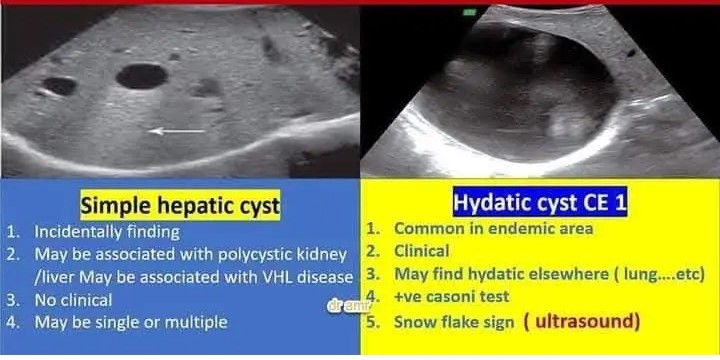
Hepatic cysts appear as anechoic (fluid-filled) structures with well-defined, smooth borders, and posterior acoustic enhancement. They are usually multiple and vary in size, often discovered incidentally on ultrasound or CT scans. Simple cysts are typically asymptomatic and don’t require treatment unless they become large and cause symptoms.
Sonographic features of simple hepatic cysts:
- Anechoic: The cyst appears black on the ultrasound image, indicating a fluid-filled space.
- Well-defined borders: The edges of the cyst are clearly delineated.
- Smooth margins: The borders of the cyst are smooth and not jagged.
- Posterior acoustic enhancement: The ultrasound wave’s travel through the cyst and are reflected back, creating a stronger echo beyond the cyst (posterior acoustic enhancement).
- Increased through-transmission: More of the ultrasound waves pass through the cyst compared to the adjacent liver tissue.
Clinical Significance and Management:
- Most simple hepatic cysts are asymptomatic and require no treatment.
- Large cysts can cause symptoms: like pain, bloating, or nausea.
- Complicated cysts: (hemorrhagic, infected) can cause pain, fever, and may require intervention.
- Differential diagnosis: Sonography can help differentiate simple cysts from other cystic lesions like abscesses or cystic neoplasms.
- Management: Small, asymptomatic cysts are often monitored. Larger or symptomatic cysts may require drainage, marsupialization, or surgical resection.
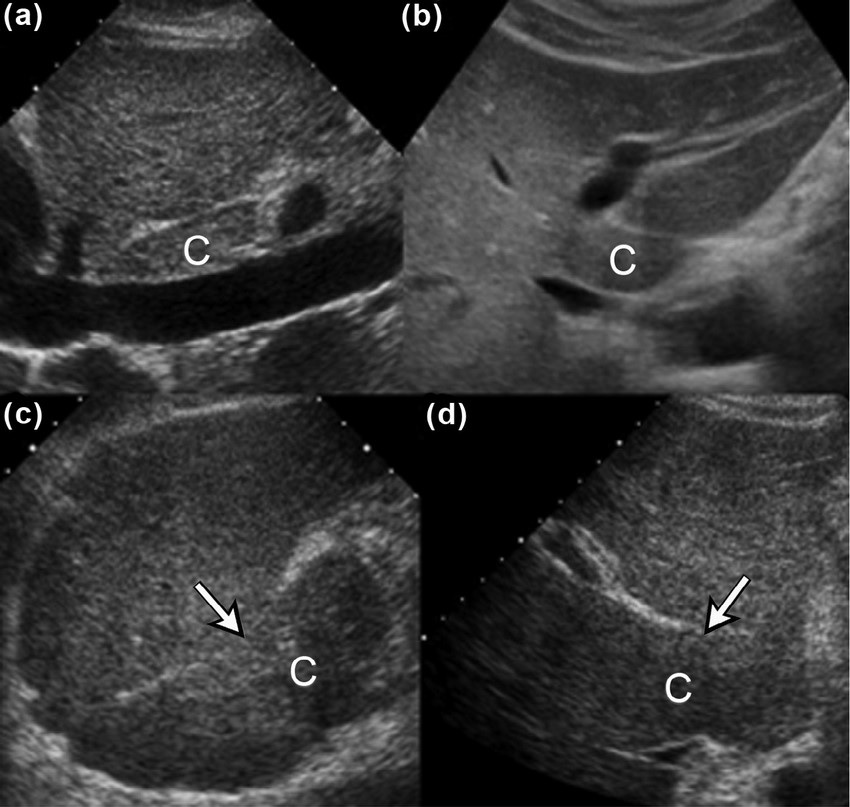
Cases
Case 1

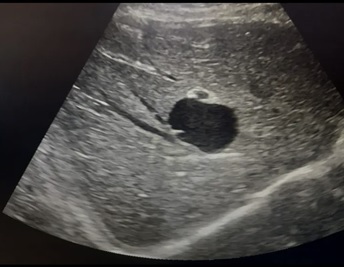
Sonographic findings: an anechoic cystic mass with a thin wall and well defined borders is seen at lateral segment of the liver
Impression: sonographic findings are suggestive of a hepatic cyst
Case 2

Sonographic findings: an anechoic cystic mass with a thin wall and well defined borders is seen at segment 5&6 the right lobe of the liver
Impression: sonographic findings are suggestive of a hepatic cyst
Case 3
History: A 60year old male complains of an epigastric pain

Impression: sonographic findings are suggestive of a simple hepatic cyst
Case 4
Sonographic findings: an anechoic cystic mass with a thin wall and well defined borders is seen left lobe of the liver
Impression: sonographic findings are suggestive of a hepatic cyst